Approved by
Chief Medical Officer of
Occupational Health Facility of
Irkutsk International Airport, OJSC
<signature>
The Role of Pulsed Travelling Magnetic Field
in Complex Treatment of Osteochondrosis
The current vertebral pathology burden in most countries reaches the proportions of an epidemic. For instance, among degenerative diseases of the musculoskeletal system, osteochondrosis (OC) of the spine not only takes the lead, but also tends for a steady increase in the number of incidence cases. Its clinical sings appear to be one of the most frequent causes of temporary disablement and often lead to permanent disability. The high expenses associated with the OC disease are also worth mentioning. Another important issue is that of medical rehabilitation of OC patients. Despite the undeniable success already made in this subject area, scientific research and development of new treatment methods for such patients are still in progress.
At present, according to evidence-based healthcare principles, the clinically essential results and outcomes of treatment should be regarded as the main criteria for assessing treatment effectiveness. This was taken as the basis for this study and for the subsequent decision to optimize the treatment process.
The findings of the study are based on the data of a comprehensive examination and case follow-up of 120 patients with neurological manifestations of OC of the lumbar spine. The diagnosis of degenerative disease of the lumbar spine was established on the basis of clinical and neurological examination of the patients, as well as on the basis of data obtained from visual and X-ray diagnostic techniques. The disease duration ranged from 2 months to 31 years, with an average value of 7.88 ± 2.10 years. Among the examined patients suffering from lumbar osteochondrosis, 63 were male (52.5%) and 57 female (47.5%), aged 20 to 63 years, the average age being 42.75 ± 0,50 years. 29 patients (24.17%) had steady-state course of the disease, while 91 (75.83%) of them had chronically relapsing one.
The reflex syndromes (RS) of lumbar osteochondrosis were registered as lumbar ischialgias and were observed in 71 patients (59.17%). Of these, 42 patients (59.15%) had right-sided, and 29 (40.85%) had left-sided lumbar ischialgia.
The ischialgias were manifested in muscular tonic, vegetatovascular, and neurodystrophic forms. The muscular tonic form of lumbar ischialgia was observed in 42 patients (59.16 %). For these patients, the muscular tonic symptoms prevailed. The vegetatovascular form was determined for 18 patients (25.35 %). This form was characterized by vasomotor defects dominating over the others. The vasospastic variation of this ischialgia form was found in 12 patients (16.9%). The vasodilatory type of vascular manifestations of lumbar ischialgia was observed in 6 patients (8.45%). The neurodystrophic form of ischialgia was registered in 11 patients (15.49 %).
Radicular syndromes (CS) of lumbar osteochondrosis were observed in 49 patients (40.83%). Among these, 41 patients (83.67%) had left-sided disposition of radicular syndrome, and 8 patients (16.33%) had right-sided one. The niveau diagnostics of patients revealed dominance of damage of the fifth lumbar root (36 patients, or 73.47%). Damage of the first sacral root was determined for 4 patients (8.16%), and damage of both the first sacral and the fifth lumbar roots was found in 9 patients (18.37%). All patients were in the sub-acute stage of the disease.
The patients were divided into 2 groups (of 40 people each) depending on the type of the treatment provided: the control group was to receive conventional treatment methods: NSAIDs by ingestion and in topical forms, massage, therapeutic exercise, stretching on “Detensor 18%” therapeutic traction mats with different degrees of hardness, wearing of a back brace (by “Orlett”) with 6 stiffeners; and the treatment group: the patients who received magneto-therapy with “ALMAG-02” device alongside with the standard treatment.
All patients were carefully examined by means of preliminary clinical, laboratory, and radiographic tests. All patients also had MRI. For all of them, osteochondrosis of varying intensity and herniated discs in the lumbar area were detected. Assessment of severity of vertebrogenic pain was performed on the basis of VAS. Severity of vertebral deformities (by means of a vertebral rotameter) and of straight leg raise were assessed. Osteoporosis of the spine, gross spondylosis deformans, ossification of the posterior longitudinal ligament were considered as complications which do not affect the course of treatment.
The following magneto-therapy method with “ALMAG-02” device was applied: With the “north” side of the main emitter facing the surface of the body, the first three exposure procedures were performed at field density of 10 mT, frequency of 3 Hz, and exposure duration of 20 minutes, with the field direction “travelling” from top downward. Beginning from the 4th procedure and up until the course end, with the same position of the emitters, the field density of 15 mT, frequency of 10 Hz, and exposure duration of 20 minutes was used.
Results of the study
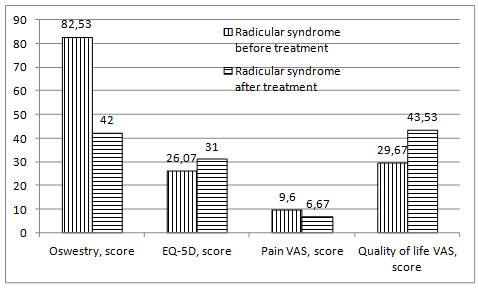
Below are the change patterns of stretch symptoms at baseline and after a course of complex differentiated treatment in the control group (Fig. 1) and the treatment group (Fig. 2) of patients having radicular and reflex syndromes.
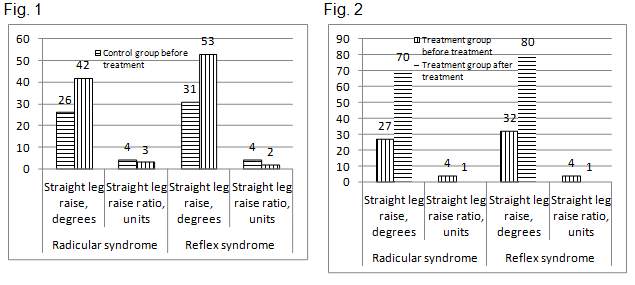
The diagrams give a visual presentation of stretch symptom features for patients of various groups throughout the case follow-up process. Straight leg raise with patients from the control group was 14.39% less pronounced than with those from the treatment group, and after completion of the treatment course the variance between the groups rose to 23.62%.
Within the control group, among the patients with radicular symptoms (RadS), the straight leg raise feature underwent a change during the treatment process amounting to 59.06%, while among the patients with a clinical pattern of reflex symptoms (RefS), the straight leg raise variance was even more pronounced and amounted to 71.89%. Straight leg raise ratio was inconsistently higher in the control group of patients with clinical aspects of RefS; upon completion of the treatment course, the studied parameter was higher for patients with clinical aspects of RadS, the variance being also inconsistent and amounting to 12.39%. The change pattern over the treatment course period for patients of the control group with RadS was 30.60%; for patients having RefS, the differences over the treatment course equaled to 41.54%. Thus, more evident changes throughout the treatment process were observed in the control group of patients with RefS.
Straight leg raise for patients from the treatment group with RadS was 19.59 % less pronounced than for those having RefS, and after completion of the treatment course the variance between the groups rose to 14.87 %. Within the treatment group of patients with RadS, over the therapy course period, an increase of the index characterizing straight leg raise was observed, amounting to151.51%, while in case of patients with RefS, the increase was 141.59%. Straight leg raise ratio was initially similar within the treatment group of patients with various clinical aspects, while after treatment, for patients with RadS, this indicator’s changes amounted to 68.42%, and for patients having RefS, the differences over the treatment course period reached 74.21%.
For purposes of comparative analysis of the values throughout the therapy course in different groups, it is important to note that patients with RadS, after the treatment course end, demonstrated growth of the parameter which characterizes straight leg raise. The largest increase of this parameter can be observed in the treatment group, where, after treatment end, the differences with the control group proved to be consistent, although this parameter value was initially comparable among the groups. Prior to treatment start, straight leg raise ratio did not differ consistently between the groups. After the therapy was provided, this index dropped in all groups, being at the minimum level among the treatment group of patients, and was consistently different from that of the control group for 55.04% respectively.
A similar trend was observed for individuals with RefS, the only difference for them being the actual variation figures. The conducted therapy revealed an increase in the parameter characterizing straight leg raise. The maximum increase in this parameter value was observed in the treatment group, where, after the treatment end, the difference with the control group proved to be statistically significant, amounting to 48.30%, while their baseline values were initially similar. Prior to treatment start, straight leg raise ratio did not differ consistently between the patients with RefS aspects. After the complex therapy was over, this index dropped in the control group and was at the minimum level in it. The difference of the relevant parameter between the treatment and the control groups amounted to 59.54.
Fig. 3. Survey data for the control group patients based on assessment performed before and after treatment.
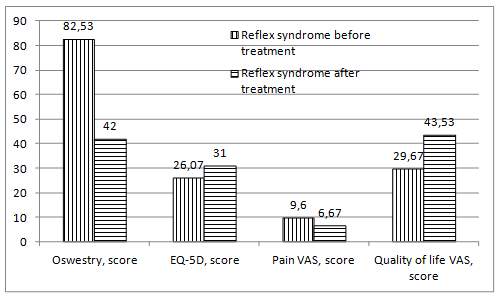
Oswestry questionnaire analysis showed that, for the control group of patients with RadS, the average score was initially higher by 24.49%. After the treatment end, a repeated survey revealed that the difference between patients with different clinical patterns became even greater, reaching 46.51%. Within their own group, the patients with RadS demonstrated a change of 55.33% over the therapy course period as per Oswestry questionnaire, while for patients with RefS the differences between the original data and the value of the studied parameter after treatment reached 68.36%. According to EQ5D questionnaire data, the initially higher values were observed among the control group of people with RefS: the difference as compared to the data of patients with RadS aspects was 69.24%. The progress of the treatment process showed an increase of the parameter under consideration. In the control group of patients with RefS, the differences as compared to baseline data were consistent and amounted to 25.20%. When comparing the data of EQ5D questionnaire after treatment, the differences between the corresponding values in the control group of individuals with different clinical patterns exceeded the original values and reached 78.19%. The survey of the pain syndrome using VAS demonstrated that for patients with RefS aspects the value in question was 22.08% lower than for those with RadS aspects. The change of the parameter indicating the pain syndrome over the treatment course amounted to 30.52% for patients in the control group with RadS aspects, and to 53.48% for patients with RefS aspects. VAS data comparison for patients of the control group with different clinical patterns showed an increase of the differences between the parameter under review to 47.83%. VAS analysis of the quality of life for individuals in the control group revealed that the baseline average score of this questionnaire was higher for patients with RefS aspects, and the difference equaled to 55.71%. Within the control group with RadS aspects, the changes in the quality of life indicator amounted to 46.71%, and for patients with RefS aspects the changes in the course of treatment were somewhat lower: 36.62%.
Fig. 4. Survey data for the treatment group of patients before and after treatment.
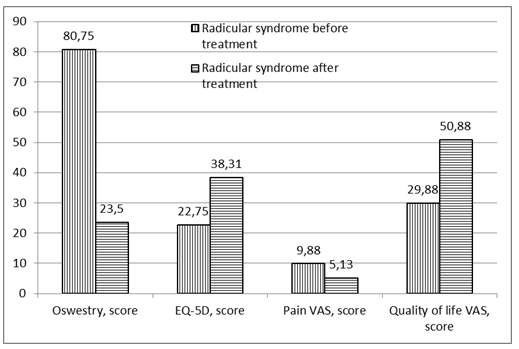
Parameters as per the questionnaires considered among the treatment group individuals are given in Fig. 4. For instance, for the patients of the treatment group, according to Oswestry questionnaire, the average score was 22.54 % higher in case of RadS presence. After treatment completion, a repeated survey showed that the difference between the indicators for patients with different clinical patterns already amounted to 65.96%. Within their own group, the patients with RadS demonstrated a change of 70.90 % over the therapy course period as per Oswestry questionnaire, while for patients with RefS the differences between the original data and the value of the parameter after treatment reached 87.21 %. According to EQ5D questionnaire data, the initially higher values were observed among the treatment group of people with RefS: the difference as compared to the data of patients with RadS amounted to 61.63 %. Throughout the course of treatment, in the treatment group of patients with RefS, the differences as compared to the original data were 61.10%, and in case of patients with RadS they were 46.42%.
Analysis of the survey data as per EQ5D questionnaire after treatment showed that the differences between the respective values of the treatment group of patients with different clinical patterns were at the level of 77.39%. The pain syndrome as per VAS for the treatment group of patients with RefS aspects was somewhat less pronounced: the difference with the corresponding value in case of patients with RadS was 25.91%. The change of the parameter indicating the pain syndrome over the treatment course amounted to 48.08 % for patients in the treatment group with RadS aspects, and to 68.31 % for patients with RefS aspects. VAS data comparison for patients of the treatment group with different clinical patterns showed an increase of the differences between the parameters under review to 54.78 % after course completion. Regarding the quality of life survey according to VAS for patients from the treatment group, it was recorded that the average score was higher for patients with RefS aspects, the difference amounting to 62.48%. The changes within part of the treatment group who had RadS, as related to the quality of life level, were 70.28%, and for patients with RefS aspects it was 62.53%.
Regarding the comparative analysis of the survey data changes in course of the treatment process, it is important to note that the average score as per Oswestry questionnaire in all groups of patients with RadS was decreasing significantly. At baseline, for all patients with RadS, the survey results as per this questionnaire were comparable. After the treatment was over, differences were notable, since the maximum level of changes was demonstrated by patients from the treatment group. In this group, the average score was 36.26% lower after the treatment than that in the control group. According to EQ5D questionnaire, prior to treatment start, all groups had comparable values of this parameter.
Following the conducted therapy, the greatest changes were observed in the treatment group, where the difference as compared to the control group’s data after treatment was 23.58%. The VAS value of pain at baseline among patients with RadS did not differ significantly between the groups. After treatment course completion, a positive trend was observed, which was most vividly pronounced in the treatment group, the difference between this group and the control group being 23.09% as related to the parameter under review. On the contrary, the quality of life VAS improved for patients with RadS after receiving a full treatment course. Accordingly, the parameter value after treatment among patients from the treatment group was 16.88% higher than in the control group, although the initial data were comparable. Thus, according to the survey data of patients with RadS aspects as per the QoL questionnaires presented, the maximal effectiveness of the treatment course was achieved in the treatment group.
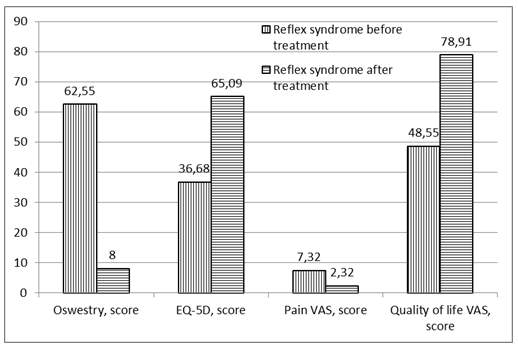
At the same time, description of the QoL survey results for patients with RefS is given in Fig. 4. Subsequently, in accordance with Oswestry questionnaire, the average score in all groups of individuals with RefS aspects was consistently decreasing during the therapy course. Primary surveying showed comparatively similar results for all patients with RefS. After the treatment, significant differences were registered, and the maximal changes were observed among the treatment group patients. The average score among patients from the treatment group after treatment completion was lower than that of patients from both groups, at the level of 59.43 and 41.82% respectively. Regarding the patients with RefS, according to EQ5D questionnaire, the baseline value of the total parameter was comparable in all groups. Upon treatment completion, the greatest changes in the reflex symptoms were observed within the treatment group, where the difference as compared to the control group’s data after treatment was 17.83%. Based on the survey data using VAS, the pain syndromes in case of patients with RefS had a similar pattern, and no significant differences were observed. After therapy completion, a reduction of this parameter value was observed, which was most vividly pronounced in the treatment group, the difference between this group and the control group being 33.33% as related to the parameter under review. At the same time, the quality of life indicator as per VAS improved for individuals with RefS after they finished their treatment course. The total VAS parameter value after treatment among patients from the treatment group was significantly (25.02 %) higher than in the control group, although the initial examination data were comparable. Consequently, according to the survey data of patients with RefS as per the questionnaires used, the maximal effectiveness of the treatment course was achieved in the treatment group.
Thus, it is important to note that the assessment of the treatment group’s results after the conducted treatment course, which involved usage of magneto-therapy of certain parameters as part of the therapeutic process, proves the need for and advisability of usage of the developed therapeutic algorithm based on the methodology applied in hospitals and in out-patient care. This is indicative of reliable expediency of the proposed care of patients having reflex and radicular syndromes of lumbar OC, provided that the suggested rehabilitation treatment complex is followed through.
Conclusions
The applied treatment complexes are effective; however, the usage of low-frequency magneto-therapy with “ALMAG-02” device has significantly increased the positive trends of the patients’ condition. Importantly, magneto-therapy was well-tolerated by all patients, and no refusals to participate in the study due to magneto-therapy intolerance were recorded. Magneto-therapy as an effective, safe and up-to-date medical factor can be successfully applied as part of therapeutic complexes for patients suffering from spinal osteochondrosis, both under in-patient and out-patient treatment conditions.
Head of
Physiotherapy Department Liliya Avimovna Sugonyako